



30th September, 2015
Combination of exclusive breastfeeding and the use of anti-retroviral treatment can significantly reduce the risk of transmitting HIV to babies through breastfeeding
Oluremilekun Osobu-Asubiojo

Photo: Oluremilekun Osobu-Asubiojo
Mariam Agboola was tested positive for HIV during her ante-natal clinic services in her first pregnancy. The news was a big surprise to her but as soon as she got home she related the information to her husband who was also shell shock. Both of them had no prior knowledge or information on the issues of HIV/AIDS.
After several counsel to clarify the uncertainty, her husband submitted himself for a test which turned out HIV negative.
However, along the line, she realized that there was some challenges that she needed to tackle. After the delivery of her baby, she was faced with the problem to sort the mix-up between the options of breastfeeding the baby or adopting a milk substitute. Knowing the essential importance of exclusive breast feeding for herself and her baby, having sought advice at the Prevention of Mother-To-child –Transmission, programme, PMTCT, she decided to breastfeed her baby exclusively.
Unfortunately, when she travelled to visit her mother-in-law, she observed that her daughter-in-law not giving the baby some water.
She could not understand the reason why she was not giving the baby water, which was of course was part of breast feeding.
She then insisted that water should be given to the child. All attempts to explain the situation to her proved abortive.
Her mother-in-law regarded her action as a taboo and refused to nurse her baby but she travelled back home and strictly followed the PMTCT guidelines recommended for prevention of mother to child transmission of HIV.
After some weeks, HIV test and confirmatory test were carried out on her baby consecutively and the news was that her baby tested negative to HIV.
She expressed her gratitude for the PMTCT programme and now has two children who are HIV negative.
“Through counseling, drugs and other handy information received on prevention of mother to child transmission of HIV, I have been able to move on. I was successfully delivered of my two children,” she said, adding that, “to me, adherence to the anti-retroviral (ARV) drugs was a great challenge and the option I opted for to breastfeed my baby exclusively without mixing baby food,” she said.
“I’m happy I benefited from the exercise. I feel happy that I was able to scale through,” she explained.
A similar story is that of Favour Iduma a 43-year old teacher who discovered she had contacted HIV in 2000.
When she suffered from what appeared to be diarrhea coupled with constant vomits, she visited the hospital for treatment. In the hospital she met a doctor friend who attended to her. The doctor advised her to go for a HIV test.
She was then encouraged to undergo a test and was told to come back for the result in three days.
On the third day, she took the sealed envelope to the doctor and the doctor revealed to her she was HIV positive.

A HIV/AIDS carrier explains the effect of mother-to-child-transmission
Photo: Oluremilekun Osobu-Asubiojo
She explained to the doctor that it could not be true and she rejected the report despite doctor’s advice. She left without adherence to treatment and HIV management. But she constantly suffered from diarrhea.
In 2004, she got married to a man who was HIV-negative. In 2006, when she was down with malaria coupled with vomiting and defecation, she was rushed to the hospital, which in turn, referred to another hospital. She was fine for a while.
But in 2009 she got pregnant with the aid of prevention of mother-to-children –transmission HIV programme. She was delivered of a baby boy. She chose to breastfeed her baby for six months. Having realized that exclusive breastfeeding builds the immune system which will be of great benefit for her baby to fight infections and other diseases.
But it was after total submission for treatment she realized she could have children, live a normal life for many years.
“HIV is not the end of life. There are many diseases that kill instantly but with HIV, one can still live for many years and have children, now, my son is five years old, he is intelligent, smart and he is disease and infection free,” she said.
He is HIV negative. I breastfed him exclusively for six months in addition with ARV drugs. I am enjoying all round benefit of breastfeeding and the PMTCT-programme. I advise people to know their HIV status and mothers to exclusively breastfeed their babies either they are HIV-negative or HIV-positive ,” she urged.
Similarly, Lucy Attah, got to know about her HIV status in 1998. She was pregnant and had to go for ante-natal at a hospital in Lagos. It was at that hospital she tested positive to HIV. She described that moment as the most horrifying and devastating moment of her life because she never believed she could have tested positive to HIV.
Though she had at one time or the other heard that the virus kills, but she had never seen anyone living with it at that time; and as such she did not know who to meet or where to go. She started gathering materials that would help her to know about the virus. She read books, articles, bulletins, and pamphlets. She read virtually anything she saw on HIV/AIDS. She experienced an inwardly-personalized stigmatization and all sorts of stigma and discrimination from some people around her.
In 2000, in seeking for knowledge on the virus she travelled to Durban for an AIDS event, where she met a lot of people from different countries who shared their experiences. This gave her courage and hope to move on to enlighten people in Nigeria on the virus.
“Being a person living with HIV/AIDS is not the end of the world; it is just a normal disease. But if it is properly managed with a healthy life style, one stands a chance of high success rate.
“People living with HIV/AIDS can get married and have children that are negative. As for me I made sure I took all preventive measures to prevent against mother-child-transmission of HIV. I have three children that are negative. My first child is 13, the second is 11, while my third child is three,” she explained.
Mother-to-child transmission, MTCT of HIV remains a major public health problem worldwide, especially in developing countries where over 95 per cent of people are living with HIV/AIDS (PLHA).
Also worldwide mothers living with HIV also face the fear of transmitting the virus to their babies through breastfeeding which has is evidently proven as an infection-free process to embark with great benefits.
Mother-to-child transmission which is when an HIV-infected woman passes the virus, can occur during pregnancy, labour and delivery, or breastfeeding.
Without treatment, around 15-30 per cent of babies born to HIV-infected women will become infected with HIV during pregnancy and delivery.
A further 5-20 per cent will become infected through breastfeeding. In 2010, around 390,000 children under 15 became infected with HIV, mainly through mother-to-child transmission. About 90 per cent of children living with HIV reside in sub-Saharan Africa where, in the context of a high child mortality rate, AIDS accounts for 8 per cent of all under-five deaths in the region.
HIV-Is the shortened form of Human Immunodeficiency Virus Sometimes called ‘‘AIDS VIRUS’’. It was discovered in 1983. The virus destroys the human defense mechanism, immunity that fights diseases, manifesting in various collection of symptoms and signs from the infections. In rapid or slow progression or sometimes no development of immune deficiency that eventually leads to AIDS, without intervention.
A person is diagnosed with AIDS when the immune system has been infected with Human Immunodeficiency.
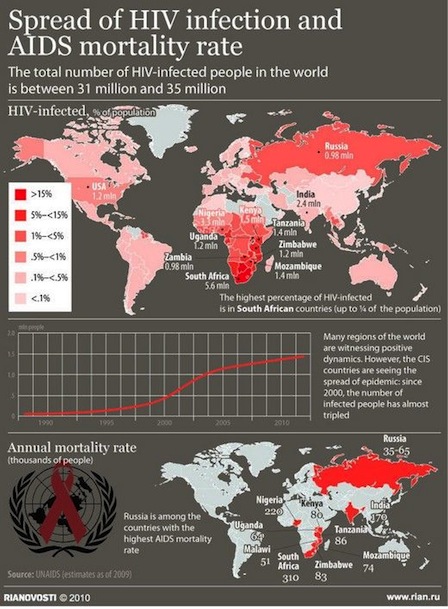
The World Health Organization, WHO, records revealed for the year 2008 and affirmed there are now 33.5 million people living with HIV.
An estimated 2.7 million were newly infected with the virus and two million died in 2008.
Dr. Nkiru David, Chief Research Fellow, Nigeria Institute of Medical Research Yaba, Lagos, explained that once the baby is born it is recommended the baby should be placed on anti-retroviral drugs as from the time of delivery up to six weeks and the mother continues on the drugs throughout the breast feeding period to prevent mother to child transmission.”
“In 2009, WHO recommended that HIV-positive mothers and their infants take anti-retroviral drugs throughout the breastfeeding, until the infant is 12 months old. For the child to benefit from breastfeeding with very little risk of becoming infected with HIV.
Research has since emerged, particularly from South Africa that a combination of exclusive breastfeeding and the use of anti-retroviral treatment can significantly reduce the risk of transmitting HIV to babies through breastfeeding.
Prior research also show that exclusive breastfeeding in the first six months of an infant’s life is associated with a three to four fold decreased risk of HIV transmission compared to infants, who were breastfed and also received other milks or foods. WHO recommended that mothers, regardless of their HIV status, practice exclusive breastfeeding – which means no other liquids or food, are given – in the first six months.
After six months, the baby should start on complementary foods. Mothers who are not infected with HIV should breastfeed until the infant is two years or older.”
David said in low income countries, which includes Nigeria, WHO recommended that: “Anti-retrovirals are taken through the pregnancy and breastfeeding stages, there is a reduction in HIV infection rate of two per cent. But there must be 100 per cent adherence to taking the drugs correctly; otherwise there is a risk that the baby will become infected with HIV or resistant to the medication. And provision of good support groups or peer groups that preach to mothers to help them adhere to an extended drug regimen as well as keeping to six months of exclusive breastfeeding is of great importance,” she said.
According to the World Health Organization (WHO) 2006 guidelines, the recommended course of drugs for preventing mother to child transmission (PMTCT) in resources-limited settings should be a combination of Zidovudine ,AZT and single dose nevirapine, NVP.
This approach is much more difficult to administer than the single dose nevirapine, but it is also significantly more effective, and is less likely to lead to drug resistance. AZT was first shown to reduce MTCT rates in 1994, and is the best-studied drug for this purpose.
David argued that breast milk however stands a better option.
WHO recommends mothers worldwide to exclusively breastfeed infants for the child’s first six months to achieve optimal growth, brain and general body development.
Thereafter, they should be given nutritious complementary foods and continue breastfeeding up to the age of two years or beyond.
The advantage of exclusive breast feeding include a lower risk of gastrointestinal infections for the baby, more rapid maternal weight loss after birth, and delayed return of menstrual periods.
No adverse effects on growth and brain have been documented with exclusive breastfeeding for six months. Numerous studies from around the world have shown that stomach viruses, lower respiratory illnesses, ear infections, and meningitis occur less often in breastfed babies and are less severe when they do happen.The main immune factor at work here is a substance called secretory immunoglobulin A (IgA) that is present in large amounts in colostrum, the first milk your body produces for your baby.
Secretory IgA substance guards against invading germs by forming a protective layer on the mucous membranes in your baby’s intestines, nose, and throat.
Breastfeeding may also help children avoid a host of diseases that strike later in life, such as type 1 and type 2 diabetes, high cholesterol, and inflammatory bowel disease.
In fact, people given breast milk as babies are less likely to have high blood pressure by the time they are teenagers.
For babies who are not breastfed, research have documented a link between lack of breastfeeding and later development of Crohn’s disease and ulcerative colitis.
Breastfeeding can protect your baby from developing allergies immune factors such as secretory IgA that is only available in breast milk.
Breastfeeding boost your child’s intelligence and this has been proven by various researchers. They found out that there is a connection between breastfeeding and cognitive development.
In a study of more than 17,000 infants followed from birth to 6 years, researchers concluded from IQ scores and other intelligence tests that prolonged and exclusive breastfeeding significantly improves cognitive development.
Experts say that the emotional bonding that takes place during breastfeeding probably contributes to some of the brainpower benefits, but that the fatty acids in breast milk may play the biggest role.
Breastfeeding may protect your child from obesity. Breast milk is the ideal food for any baby, for the best growth and development mentally, emotionally and physically. It is not only important for a baby, but has many benefits for the mother, namely: helping her lose the postpartum pounds easily after birth, it also helps prevent postpartum depression. Breastfeeding may reduce your risk of some types of cancer such as breast and ovarian cancer. For breast cancer, nursing for at least a year appears to be the most protective effect.
It’s not entirely clear how breastfeeding helps, but it may have to do with the structural changes in breast tissue caused by breastfeeding and the fact that lactation suppresses the amount of estrogen your body produces. Researchers think the effect on ovarian cancer may be related to estrogen suppression as well.
Futhermore, on HIV and the the prevention of mother to child transmission, Dr. Oliver Ezechi, Clinician obstetrician and gynaecologist at Nigerian Institute of Medical Research, Yaba, identified HIV subtypes in a programme organized by Journalist Against Aids, JAAIDS in collaboration with World Association For Christians Communication, WACC.
Dr. Ezechi Identified HIV1 and HIV2 subtypes, to be highly variable viruses which mutates very readily.
This means that there are many different strains of HIV, even within the body of a single infected person.
He stated that HIV 1 is characterized by high rate of replication, circulation and more dangerous compared to HIV 2. The replication which is highly prone to errors, gives rise to several mutants.
HIV 1 is commonest globally while HIV2 is restricted to the West, but in Nigeria it is variant.
The UNAIDS report on Nigeria revealed that Nigeria has the third largest number of HIV infections in the world with roughly four million men, women, children and youth. Nigeria also has the highest prevalence of HIV/AIDS between age group of 15 and 24.
WHO, record revealed that half of all new HIV infections occur among young people, aged 15–24. In 2007, an estimated 33.2 million people were living with HIV, 5.4 million of whom were aged 15–29 years.
Speaking on the prevalence of HIV/AIDS by age group, Dr. Ezechi also pointed that a 2005 survey revealed that the highest prevalence of HIV was among people between 15-29 years with the percentage of 4.9 per cent among other groups
In sub-Saharan Africa, there are 3.2 million young people living with HIV, with a ratio of three young women infected for every young man, citing female anatomy as the reason for this.
He noted that the transmission rate of male to female is faster than female to male because the man’s semen is deposited in the woman. He also added the social-economic factor known as “Aristo or runs syndrome”, which is; when young ladies depend on older men for financial support with demand for sexual pleasure in return, amid other factors.
Dr. Ezechi expressed his concern on the magnitude of Mother-To-Child-Transmission, MTCT, in Nigeria, MTCT based on research. He said that there are about 6 million pregnancies in Nigeria per year. And 4.1 per cent HIV prevalence in pregnancy and about 250,000 HIV positive pregnant women and 30- 40 percent Mother–child-transmission without intervention.
While Dr. David, identified the factors responsible for the large burden of transmission of mother-child-transmission of HIV, MCTC , in Nigeria to be as a result of the large population, individual inability or unwillingness to know their HIV-status.
And access to antennal service outside the organised medical care that do not have access to the Prevention of Mother-To-Child-Transmission, PMCT package also pose a problem.
She mentioned that despite the PMTCT programme that is being scaled up from the tertiary institution to secondary and primary health care facilities with the collaboration with traditional birth attendants’ women still give birth in mission homes among others, she said.
She advised on the need for every woman to know her HIV-status before marriage, before getting pregnant and while pregnant and to access PMTCT programme if she is tested positive to HIV. So as to have children who are free of HIV for better tomorrow.
As a means to prevent of mother-To-Child-Transmission, Dr. Ezechi mentioned that to prevent HIV infection among prospective parents – making HIV testing and other prevention interventions available in services related to sexual health such as antenatal and postpartum care and focusing on preventing HIV in women of a child-bearing age.
She added that HIV positive women should avoid unwanted pregnancies. Provision of appropriate counseling and support to women living with HIV to enable them to make informed decisions about their reproductive lives by ensuring that contraception is available to women who want it.
And prevention of transmission of HIV, from HIV positive mothers to their infants during pregnancy, labour, delivery and breastfeeding.
Integration of HIV care, treatment and support for women found to be positive and their families.
Dr. Ezechi emphasized that for HIV positive mothers and those women who seemed unqualified for anti-retroviral drugs due to high immunity but are still positive should be on drugs as soon as they are pregnant so as to protect the baby from the viruses and also that they ensure to embark on adequate safe delivery service and practice which involves observing the woman in labour making sure that the mother does not rupture the membrane more than four hours before the baby comes. And then primarily knowing the viral load which is the level of the viruses in the women’s body.
Dr Ezechi stated that if it is above 1000 copies/ml, the woman can safely have vaginal delivery.
However if the copies are above 1000 is might be safer to have operative delivery.
He warned HIV-positive mothers and people living with HIV to religiously take their drugs to prevent drug resistance that can lead to drug failure and death.
“We have witnessed family friends, pastors and imams who have persuaded patients not take their drugs. This is extremely dangerous and detrimental because faith without works is dead”.
For Dr David, he advised mothers that tend to replicate the western behavioral pattern of positive mothers who do not engage in the act of breast feeding to opt for breast milk substitutes if they choose to over look social-environmental factors associated to breastfeeding act.
She noted that such mothers must be financially, hygienically and adequately prepared to meet the baby’s nutritional needs.
She warned mothers have chosen or want choose the option of baby substitute to strictly feed the baby with baby formula alone.
“The combination of breast milk and formula is the most dangerous thing you can do to your baby. It is associated with increase rate of transmission, it should never be done. That is why we counsel mothers when they are pregnant to decide on the options available”.
Dr. Ezechi stated that HIV/AIDS prevalence constitute the greatest challenge of our time. “For this reason it must the responsibility of all sectors which also includes the churches and mosques to educate teenagers, youths, men and women on HIV/AIDS on how HIV is spread, how it can be prevent and managed to reduce the its scourge in the society ’’
Speaking on the spread of HIV, Dr. Ezechi disclosed that HIV can be spread through semen, vagina and cervical secretion, amniotic fluid, synovial fluid around bone joint, breast milk, re-using and sharing of needles and sharp objects, unprotected sex, mother-to child and unscreened blood transfusion.
“Prevention is better than cure, HIV/AIDS can be prevented through total abstinence, faithfulness to one’s partner, use of condom and by refusing to share of sharp objects,” he stressed.
With great concern for the future generation, Dr. Ezechi advised people who at one time or the other had never undergone voluntary testing for HIV/AIDS to do so for their own good to know their status.
And if they are negative they will know how to live their life as being negative by maintaining the practices of being negative but if they are positive, they can access care so they can remain healthy and live a healthy life style.
Dr. Ezechi also spoke on the wrong perception of people who still believe that HIV is spread through sweat, shaking of hands and eating from the same plate.
He said all these misconception are untrue and he emphasized that “everybody should undergo voluntary testing to know their HIV/AIDS status, as AIDS does not show on the face.